October 29, 2015
From paper to pixels — the new paradigm of electronic medical records
Transitioning to electronic health records introduced new approaches, skills, and understandings of patient records, improving the care experience.
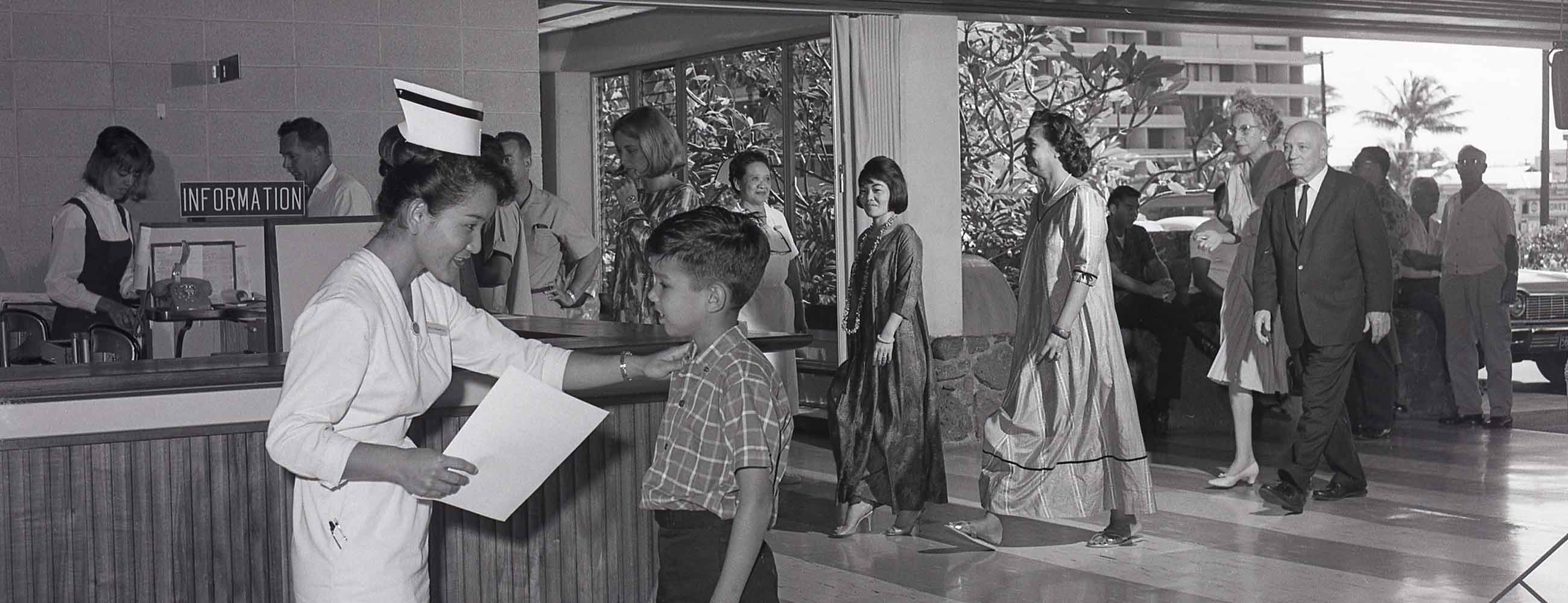
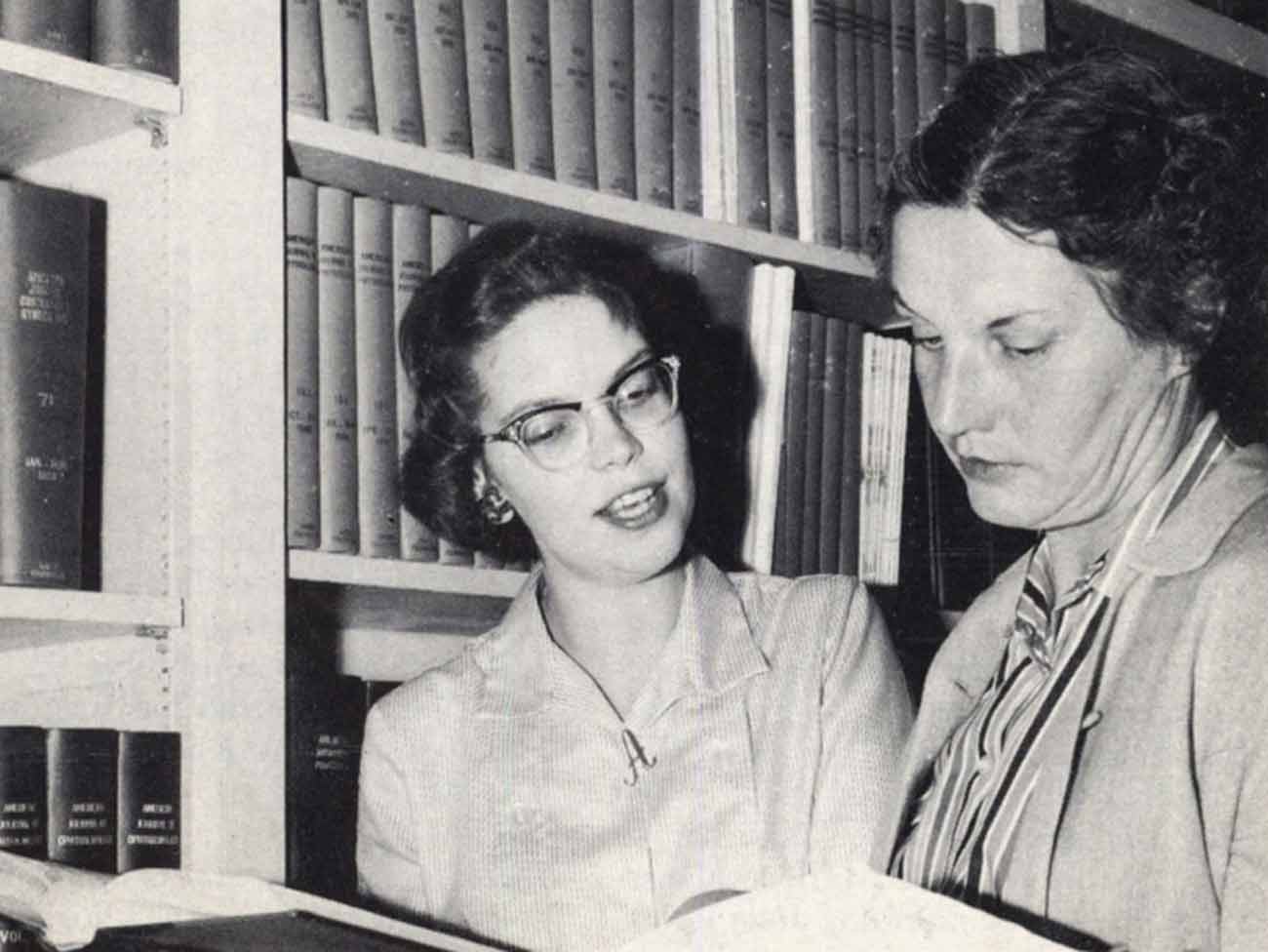
Bess Kaiser Hospital medical record department, 1959. Receptionist in foreground identifies desired patient folder to be pulled from shelves in background; pneumatic tubes deliver files to nursing station.
Change rarely comes easily. People get used to doing things a certain way, and physicians are no exception. One such shift was a technology Kaiser Permanente adopted early on, creating patient medical records electronically rather than on paper.
In 2013 I interviewed Jim Gersbach, senior hospital communications consultant for Kaiser Permanente’s Northwest region. As their unofficial historian, Jim had accumulated many stories during his 28 years of service. This is an edited version of one of his learnings.

“EpiCare was forcing [doctors] to actually enter data on every patient; they couldn’t just leave it blank.” — Jim Gersbach
I can remember some of the older doctors didn’t even know how to type. That was the biggest barrier; they were doing the old hunt-and-peck because they had never needed to type. They just did dictation, or their nurses would type it up for them. The younger physicians were very eager to adopt computerized medical records because they were a little bit more familiar with computers.
But after 1998 the Northwest Permanente Medical Group had done some survey work — [which had some] pushback — and heard that ‘This is adding to our day; it’s 45 minutes more a day to try and enter all this stuff in.’ People were complaining that ‘When I did paper, I didn’t take so long to do all this stuff, so it’s not a time saver for us.’
We started looking at that and found that sometimes when doctors would get busy, they would just sort of scribble something illegible in the chart, and send it off because they could get out of their office faster. EpiCare was forcing them to enter data on every patient; they couldn’t just leave it blank. That was a major ‘Aha!’ moment. What became evident was, ‘Wait a minute; we’re not necessarily charting everything we’re supposed to.’ And the computerized system helped.
Not only did it make everything legible, but it forced clinicians to put something in; you had to type something in, or it wouldn’t advance you forward. It improved the quality of the data.
In the Northwest, at the time EpiCare was being adopted, the doctors were very free to say what they didn’t like about it. But despite all the grumbling about ‘It’s adding to our length of the day,’ when we asked, “Would you ever want to go back to paper?” they said ‘Absolutely not! I couldn’t live without the system, because it provides me everything I need to know for the patient.’ They very quickly saw the value of it as a clinical aid.